We learned in
Lynn's
story that she was born and raised as a boy, and later in
life was changed into a girl by female sex hormone treatments
and major surgical procedures. Because of this past, Lynn is
sometimes called a "transsexual" woman. Why did this
happen to Lynn, and what is transsexualism anyway?
In Part I, we first answered
some basic questions about gender and transgenderism. We learned
about the nature of gender identity, about where it comes from
and about what events occur in nature that interfere with correct
assignments of gender. We also learned about transgenderism and
transgender (social) transitions.
Here in Part II, we provide
detailed information about MtF transsexualism, including historical,
cross-cultural and prevalence information. We also describe current
methods and technology for complete MtF transsexual transition,
and provide links to more information about TS (social and physical)
transition.
Then, later in Part III,
we discuss the lives of women after MtF transsexual transition.
Many short term practical issues face these women, and they also
must manage longer term issues such as living in stealth vs being
open about their pasts, adjusting or severing post-transition
relations with family, relatives and former friends, dealing
with a variety of legal issues, obtaining compassionate health
care, finding good employment and managing their careers, adjusting
to their new sexuality, finding and maintaining love relationships,
and achieving full social assimilation as a woman.
Knowledge in this area is under rapid development. The taboo
on this area has also been broken, so that we can openly discuss
these important issues without fear, shame or embarrassment.
Much more is known about transsexualism and methods for transsexual
transition than just a few short years ago, and those new understandings
are very much worth sharing and building upon. Far more people
suffer from transsexualism than previously suspected. The key
to improving the quality of their lives is better knowledge and
more widespread understanding of all this emerging knowledge.
The great obstacle to transition: The challenge of confronting
and coping with fear
Fear is often heightened by GLBT activism which portrays
all TG's & TS's as "victims"
WARNING: Be sure to visualize the real risks of transition
and factors that affect success
Assessing risks, making decisions, and taking actions
during transition
How can family, friends, teachers and co-workers help
a transsexual woman in transition?
With better understanding, how might transsexualism
be treated someday?
TS Success Stories: Websites of Successful Post-op TS
Women
Part II: TRANSSEXUALISM (*MtF)
Transsexuals are the most intensely afflicted of transgender people. They
strongly feel that they are, or ought to be, the physical gender opposite to
that in which they were born and raised. The body they were born with does
not at all match their own inner gender feelings and image of who they are
or want to be, nor are they comfortable with the gender role that society
expects them to play based on that body. Most are painfully aware of their
gender incongruity from very early childhood. While transgender transitioners feel compelled to correct their social gender,
transsexual transitioners feel compelled to also correct their physical gender.
If you've seen the movie Boys
Don't Cry, then maybe you can visualize the deep feelings
and passions that drive a transsexual teenager (in that case
a female to male (FtM) transsexual) into crossing over the gender
divide, the joys they feel when accepted and finding love on
the other side, and the terror and humiliations that await them
if their status is ever discovered.
The movie Different
for Girls also conveys some of the nature and depth of
early transsexual feelings, especially in its powerful and poignant
opening "shower scene". Here a young male-to-female
(MtF) teen is seen experiencing transsexual girly body feelings,
with her genitals tucked away and hidden from herself . While
in this reverie, she feels some of the joys of being a sensual
woman, at least for a little while.
Suddenly, she is set upon and violently attacked
by a group of boys
who've witnessed her behavior:
Fortunately, she is rescued by another boy who confronts
the group,
puts his jacket around her and comforts her:
This scene from Different
for Girls captures ever so much of the inner experience
of being a young trans girl, from experiencing the joys of a
blossoming female sensuality, to experiencing the dangers of
being attacked for exhibiting those feelings.
You can see in her responses in this unfolding situation,
in the lonely terror and vulnerability in her eyes, and in her
emotional release into the arms of her rescuer, that she is inherently
a girl inside - even though she exists at the time in a boy's
body. The movie well portrays the inherent femaleness of this
young trans girl, as opposed to the more exaggerated effeminacy
frequently seen in young gay boys.
For more about this scene, see Victoria Jefferies page "Boys - personal
reflection", which is located in her wonderful website
for young trans girls, "From
Within". Many thanks to Vicky for capturing these
still-images from the movie! (Note that Vicky had a somewhat
similar shower experience when she was a young teen.) Vicky's
overall website conveys in many powerful ways what it feels like
to be young and trans, and is highly recommended reading.
The behavior of experiencing female sensuality while hiding
their genitals is a very common behavior in young trans girls.
As they grow older and begin to be masculinized by testosterone,
the time may come they when no longer can conceal from themselves
and others the effects of the awful transformation being forced
upon their overall bodies. From this point onwards they may experience
intense emotional distress and anxiety.
Thus many transsexual people feel almost claustrophobically
trapped and destined to live out their lives "imprisoned
in the wrong body", unless they can correct the situation
with sex hormones, sex reassignment surgery (SRS) and complete
physical transition. They long to live out their lives in the
correct gender not just socially, but also in their private,
intimate lives too - in the right body for their inner gender
feelings.
They feel as you might if you suddenly found yourself physically
changed into the opposite gender and forced into that gender
role, while still having all the body feelings and social identifications
of your old gender. It is a profoundly disorienting experience
to have a body that is totally wrongly-sexed. Everyone is challenged
in their efforts to find love in this life. Can you imagine how
frightening and challenging that is if you were wrongly sexed?
[ *Note: In this webpage we focus on male to female [MtF]
conditions, since those are within Lynn's direct experience.
However, there is a completely symmetrical set of female to male
[FtM] gender conditions that are almost as common as MtF conditions.
For more information about FtM transgenderism and transsexualism,
see the websites of FtM International
and The American Boyz. The
article "Girls
will be Boys", by T. Eve Greenaway discusses the sudden
emergence of FtM transgenderism out of the shadows and into the
open in many U.S. colleges and universities. For in-depth background
on FtM transgenderism and transsexualism, see the recent book
by Jason Cromwell, Transmen
& FtMs. See also Lynn's webpage listing weblinks
and photos of Successful
TransMen(es). ]
Historical and cross-cultural
evidence of transsexualism
Transsexualism is not a "modern discovery". Instead
it is a not-uncommon, naturally-occurring variation in human
gendering that has been observed and documented since antiquity.
In many cultures, including native tribes in North America,
transsexuals have long had the choice to cross-dress and live
their lives as women, including taking husbands. The surgical
alteration of genitalia to relieve intense cross-gender feelings
was also not "invented in the twentieth century". In
some cultures, including many ancient ones, many transsexuals
have voluntarily undergone surgeries to modify their bodies in
such a way as to "change their sex".
The surgical methods and the effects of castration were everywhere
for the ancients to see. Its use in the domestication of animals
quickly taught ancient people that removal of a human male's
testicles at a young enough age would prevent his masculinization
too. Such a person would forever be childlike - or "girly".
These surgeries were also often forcibly done upon captive adult
male slaves in order to "domesticate them" as "eunuchs".
Performing such surgeries on normal post-pubertal males does
not change their gender feelings or gender identity, although
is lessens their sexual drives somewhat and sharply reduces their
ability to develop male musculature.
The accumulated knowledge about the effects of castration
was further extended to help MtF transsexual girls: Untold millions
of them over thousands of years have voluntarily sought and undergone
surgeries vastly riskier and more dramatic in effect than mere
castration. In these surgeries the girls are completely emasculated
by total removal of the testes, penis and scrotum. In addition,
the external pubic area is often roughly shaped to look like
a girl's vulva. No one knows precisely how it started, but such
transsexual surgeries were well known by the time of ancient
Greece and Rome. These transformations were usually traditionalized
in "religious rituals" that provided the resulting
"women" with an explanation for what they had done,
and thus a "cover story" for finding a place in society.
By undergoing these surgeries, young MtF transsexual girls
(if they survived) not only avoided becoming men, but also gained
genitalia that looked somewhat like those of a woman. Although
lacking vaginas and lacking the powerfully feminizing effects
of female sex hormones, young transsexuals in the past could
nevertheless live life better as women after undergoing such
surgery. By retaining their pretty girly features and soft sensual
skin from childhood, and by avoiding becoming hairy all over
and having craggy facial features, some of them could attract
and enjoy male lovers as women. In some societies they could
even hope to find a husband to love them and care for them.
Many skeletal remains of surgically modified transsexual
women from ancient times have been uncovered by archeologists,
who usually refer to them in confused terms as "eunuchs"
and "transvestites", as in the BBC story
"Dig
reveals Roman transvestite" about a skeleton found recently
in England. Here's an excerpt and a photo from that BBC story:
"Archaeologists in North Yorkshire have discovered
the skeleton of a cross-dressing eunuch dating back to the 4th
Century AD. The find was made during excavations of a Roman settlement
in Catterick, first started in 1958.
The skeleton - found dressed in women's clothes and jewelry
- is believed to have once been a castrated priest who worshiped
the eastern goddess Cybele. - - - The young man was found buried
in a grave at Bainesse, a farm near Catterick, and once an outlying
settlement of the Roman town.
He wore a jet necklace, a jet bracelet, a shale armlet
and a bronze expanding anklet - - - In life he would have been
regarded as a transvestite and was probably a gallus, one of
the followers of the goddess Cybele who castrated themselves
in her honour."
It is so sad when archeologists naively obscure and inherently
ridicule this girl's gender identity by calling her a "cross-dressing
eunuch". Such comments reveal their lack of understanding
of human nature in the large, and their lack of appreciation
for how sophisticated some ancient civilizations were when accommodating
gender variations. Those who are knowledgeable about transgenderism
and transsexualism will recognize that this person is not a "eunuch"
(a male-gendered boy or man who has been castrated - in ancient
times usually as a slave), nor is she a "transvestite"
(an intact male-gendered man who is cross-dressing for male erotic
satisfactions).
Instead this person was very likely an intensely transsexual
girl who desperately sought and willingly underwent a voluntary
emasculation surgery at a young age, probably her early teens,
and then lived as a female "priestess" afterwards.
The evidence that she underwent her primitive sex change early
in life is staring right out at us in the photo above: The girl
has no male brow-ridge on her forehead above and between her
eyes (take a close look at the photo above). Given her rounded
female facial structure and slight build, she may have been a
very beautiful woman. Her elaborate burial upon her death in
her early twenties suggests that she was very much beloved, and
perhaps left behind a grieving lover or patron.
These ancient practices continue in some parts of the world
even today. In India and Bangladesh very large numbers of desperate
young transsexuals run away from home to join the "Hijra"
caste. To become Hijra, these teens voluntarily undergo fully
emasculating surgeries under primitive conditions just as they
would have in ancient times, with only opium as an anesthetic.
Most undergo the surgery in their teens shortly after the onset
of puberty, with results as seen in the photo of a young Hijra
woman on Lynn's SRS webpage. By being
castrated just early enough they can avoid the development of
male secondary sex characteristics (except for the breaking and
lowering of the voice), and their bodies can remain permanently
soft, childlike and girly. These "sex changes" and
their effects are shrouded in mystery and religious symbolism.
The possibility of being able to undergo such sex-changing
transformations is widely known about in India, and exerts an
incredibly powerful and mystical calling to all young transsexual
girls there. About one in every four hundred such teenagers runs
away from home in modern India and becomes Hijra, and there are
now approximately one million of them in the country.
Contrary to popular myth, total emasculation after puberty
does not necessarily "de-sex" the young person. Castration
after puberty leaves the young Hijra with her newfound feelings
of sexual arousal and her newfound orgasmic capabilities. While
the psychological impact of such surgery would cripple the libido
of a normal male, the effect on a young transsexual girl is just
the opposite: The surgery is liberating, and enables a fuller
expression of her sensuality and libidinous feelings. Just as
in the case of modern post-operative transsexual women, many
Hijra can have strong feelings of sexual arousal in the inner
remnants of their genitalia (even though they lack the external
nerve tissue preserved by modern SRS). Although Hijra lack vaginas,
many greatly enjoy (to orgasm) penetrative (anal) sexual activities
with men. Because of their complete emasculation, Hijra genitalia
and pelvic regions look very "girly". Many men in India
greatly enjoy lovemaking with Hijra, and thus the girls can find
some small measure of intimate contact, passion and love in this
life.
Most Hijra live out their lives as women with other Hijra
in "family groups", earning an existence by performing
in traditional ceremonies at weddings and childbirths. Many work
as prostitutes and beggars in this lowest of traditional Indian
castes. Some Hijra today are fortunate to have access to female
hormones, and can feminize their bodies by growing breasts and
developing natural female body contours. The combination of emasculation
as teenagers combined with use of estrogen enables some Hijra
now to become very beautiful - even though, sadly, they do not
have female genitalia (vaginas) and are not socially accepted
as women.
The Hijra community and its traditions, including their very basic form of
"sex change" from male towards female, has a recorded history of over 4000
years in India. This widespread practice in India enables transsexual
kids
to escape the angst and fate of masculinization as teenagers,
and provides a safe though very lowly place in society for them. The
agonizing extremes to which these transsexual youngsters will
go in order to "approximately have a female gender",
with full knowledge that they will never see their families again
and will face social degradation for the rest of their lives,
is a testament to the reality and extremity of the gender conflict
that they face within themselves.
Today in India the Hijra are thought of as a "third
gender", and are often called "eunuchs" because of
the British use of that term for them. This use of the word eunuch
is a total misnomer and is very unfortunate, because that English
word has long been used to signify castrated adult males who
identify as males. The word conjures up images of loss and neutering,
rather than of feminization and the resolution of gender confliction.
Thus the word does not convey the transsexual nature of the Hijra,
and tends to further marginalize them as social outcasts.
That indeed was their fate during the period of colonial
British oppression in India. Before British rule many Hijra lived
fairly secure lives working as domestic "girls" in
the homes of wealthy people and by performing during numerous
ritual ceremonies. However, many traditional Hijra social roles
were eliminated by homophobic British colonials unable to visualize
the deep meaning of Hijra traditions. Many Indians themselves
then came to view the Hijra as "perverted" street people,
by buying into the "modern and advanced" British colonial
attitudes towards this gender minority.
In the face of caste stigmatization, the Hijra are secretive
about their surgical initiations and practices. Some say that
they were abducted and emasculated against their will, making
it seem to "not be their fault". Although they view
their emasculation surgery as a "sex change", the Hijra
are also realistic in their recognition that they are not really
women. However, they wear female clothing, take feminine names
and use female pronouns. They embrace their ambiguous status
as preferable to being men, for them. The practice is very widespread
in India and Bangladesh (see Prevalence
section, below). For more information see the Kinnar (Hijra)
website at http://www.kinnar.com/
Although shrouded in caste secrecy and mystery for centuries,
the underlying condition that compels most of the young teenagers who become Hijra is clearly transsexualism. Says Dhanam, the leader of a
Hijra family in India (i.e., a Hijra 'Guru'):
"We are born with a gender identity crisis.
It is not an imitated or learnt one,
but a natural instinct that urges us to be women.''
- Dhanam
Important note:In 2002 Lynn began to communicate with
a number of Hijra women in India, and strongly suggested that
they try wherever possible to eliminate the use of the word "eunuch"
to refer to them. Lynn suggests that they substitute the word
"transgender" or "transsexual" for "eunuch"
whenever they are using English. If the Hijra can gradually bring
about this change in English terminology in India, they would
more correctly be seen as transgender and transsexual women instead
of as some kind of weird "crossdressing-castrated men".
Such a change in viewpoint about their nature could help make
a much stronger case for the "transgender rights" of
Hijra in India.
Even in the modern western world some truly desperate young
transsexual girls who cannot find help from the medical system
will "commit Hijra" upon themselves. By fully emasculating
themselves and then falling upon the medical system for "patching
up", they can achieve a "low-cost SRS early in life".
A number of girls in the U.S. have performed these complete emasculations
on themselves, and then feminized themselves with estrogen to
quickly become very passable and pretty as girls (unfortunately,
the loss of penile and scrotal skin makes later SRS much more
difficult). These desperate acts were more common decades ago
when TS girls in the U.S. had great difficulty obtaining medical
help. An even more common practice has been for TS girls to resort
to basic self-castration (removal of their own testicles) in
order to avoid masculinization.
The Hijra are, in many ways, a long-traditionalized cultural
equivalent in India of the "street trannies" seen on
the nightime streets in many major U.S. cities, and indeed
(as "travestis") in
cities all around the world (for example, see the recent
survey of transsexuals in Malaysia).
None of these societies is aware that many of these people are
transsexuals who at heart desperately need to be women, and who,
without identification papers, social position or families, usually
have no employment options other than prostitution.
Here in the U.S., the street trannies are usually thought
of by polite society as "sexual deviants who have lost their
minds". They are very frequently misclassified as "gay"
males, when in fact they often self-identify as girls and their customers
are mostly straight guys (not gay men) who enjoy lovemaking with
"she-males". Thus both the Hijra of India and the
hormonally feminized
street trannies in the U.S. are mostly transsexuals. Both
groups are misunderstood and mis-identified by society, and treated
as male social outcasts. Instead, they are people who are just
doing the best they can to be, and to live as, women.
Photo of Pokaraji, a pretty young
Hijra girl in Calcutta, from the remarkable book
Here are photos of two other Hijra women from
Takeshi
Ishikawa's book. As you can see, some Hijra are very beautiful.
Sonamu (on the left) grew up as a street child in Bombay India,
and then became a Hijra in her teens. She was so beautiful that
she became rather famous in Bombay.
Sonamu
Patora
Important note: In September 2003, the
Peoples’ Union for Civil Liberties, Karnataka (PUCL-K) published a truly
remarkable report on human rights violations
against the transgender community in India. In the spring of 2004, I
was fortunate to obtain a copy of the report, and I wish to alert you to it via
this webpage.
The 117 page PUCL report
provides extensive background on the social, cultural and political context of Hijras. It then documents violence against
the Hijra, and discusses the institutional basis of this violence. It documents
recent Hijra efforts to organize and protest the discrimination that they face,
and makes important recommendations on how to improve the plight of transgender
people in India. The report is an excellent source of up-to-date cross-cultural
information about the Hijra, and I highly recommend it to you. See the following
webpage for more information, including links for downloading the report in PDF
format:
http://ai.eecs.umich.edu/people/conway/TS/PUCL/PUCL Report.html
What causes transsexualism?
Many causes for transsexualism have been proposed over the
years. As discussed above, it's long been known from many intersex
cases that the genes do not determine gender identity. The recent
follow-ups on intersex infant surgeries also show that "genitals
and upbringing" do not determine gender identity. Instead,
current scientific results strongly suggest neurobiological origins
for transsexualism: Something appears to happen during the in-utero
development of the central nervous system (CNS)
so that the transsexual child is left with innate, strongly perceived cross-gender
body feelings and self-perceptions. We still don't know for sure
what causes it, and more research needs to be done. But the neurobiological
direction for these scientific explorations seems clear.
For example, recent research suggests that MtF transsexualism
may result from a female differentiation in a genetic male of
the BSTc portion of the hypothalamus, during interactions between
the developing brain and fetal sex hormones; this brain region
is essential to sexual feelings and behavior. The first such
research was reported in 1995: See NATURE, 378: 60-70,
1995 (this paper is also web accessible at http://www.symposion.com/ijt/ijtc0106.htm
). Extensions of this earlier work were reported in May 2000
(see following abstract and link to the full paper) :
The Journal of Clinical Endocrinology &
Metabolism, May 2000, p. 2034-2041
Copyright 2000, The Endocrine Society Vol. 85, No. 5
Frank P. M. Kruijver, Jiang-Ning Zhou, Chris
W. Pool, Michel A. Hofman,
Louis J. G. Gooren, and Dick F. Swaab
Graduate School Neurosciences Amsterdam (F.P.M.K.,
J.-N.Z., C.W.P., M.A.H., D.F.S.), Netherlands Institute for Brain
Research, 1105 AZ Amsterdam ZO, The Netherlands; Department of
Endocrinology (L.J.G.G.),
Free University Hospital, 1007 MB Amsterdam, The Netherlands;
and Anhui Geriatric Institute (J.-N.Z.), The First Affiliated
Hospital of Anhui Medical University, Hefei, Anhui, 230032 China
Address all correspondence and requests for
reprints to: Frank P. M. Kruijver, M.D., or Prof. Dick F. Swaab,
M.D., Ph.D., Graduate School Neurosciences Amsterdam, Netherlands
Institute for Brain Research, Meibergdreef 33, 1105 AZ Amsterdam
ZO, The Netherlands. E-mail: F.Kruijver@nih.knaw.nl.
Abstract
Transsexuals experience themselves as being
of the opposite sex, despite having the biological characteristics
of one sex. A crucial question resulting from a previous brain
study in male-to-female transsexuals was whether the reported
difference according to gender identity in the central part of
the bed nucleus of the stria terminalis (BSTc) was based on a
neuronal difference in the BSTc itself or just a reflection of
a difference in vasoactive intestinal polypeptide innervation
from the amygdala, which was used as a marker. Therefore, we
determined in 42 subjects the number of somatostatin-expressing
neurons in the BSTc in relation to sex, sexual orientation, gender
identity, and past or present hormonal status. Regardless of
sexual orientation, men had almost twice as many somatostatin
neurons as women (P < 0.006). The number of neurons in the
BSTc of male-to-female transsexuals was similar to that of the
females (P =3D 0.83). In contrast, the neuron number of a female-to-male
transsexual was found to be in the male range. Hormone treatment
or sex hormone level variations in adulthood did not seem to
have influenced BSTc neuron numbers. The present findings of
somatostatin neuronal sex differences in the BSTc and its sex
reversal in the transsexual brain clearly support the paradigm
that in transsexuals sexual differentiation of the brain and
genitals may go into opposite directions and point to a neurobiological
basis of gender identity disorder.
However, without even having ANY scientific evidence to back
them up, many psychiatrists and psychologists over the past four
decades have simply assumed that transsexualism is a "mental
illness". By DEFINING this socially unpopular condition
to be a mental illness, psychiatrists have shaped much of the
medical establishment's and society's view of transsexuals as
"psychopathological sexual deviants". However, those
viewpoints are gradually fading away as the old generation of
traditional "behaviorist" psychiatrists passes on,
and as the underlying neurobiological bases for many basic human
behaviors have begun to be understood.
For a more complete discussion of the older "mental
illness" concepts of transsexualism, and a comparison with
more recently emerging scientific evidence for neurobiological
causes, see Lynn's page on
Do we really need to know
the cause in order to treat the condition?
Why is there so much fixation on "causes"? The
answer is simple: Transsexualism has been such a socially unpopular
condition in the past that the issue of "what causes it"
is always raised in discussions about what to do about it. In
the past many behaviorist psychologists and psychiatrists have
inherently blamed transsexuals for causing their own "sexually
deviant mental illness", giving those psychiatrists a claim
to responsibility for the "treatment and cure of transsexuals"
and giving society a rationale for discrimination, marginalization
and ghettoization of transsexuals.
However, as we've seen, transsexualism is most likely a neurological
condition of as yet unknown origin and not a "mental illness".
There are many other intense neurological conditions such as pain,
depression and bipolar disorders for which we do not know the
underlying causes but suspect biological causes. We know that
these other conditions are real because we see people in distress,
and we treat those people medically and with compassion to relieve
their suffering.
Why should it be any different with transsexualism?
We now know how to relieve the suffering of transsexual people,
having many options for practical counseling, social transition
and hormonal/surgical gender reassignment. Why not accept those
treatments as valid, since they truly relieve suffering and enhance
the quality of life, even if we aren't sure what causes the underlying
condition? And why stigmatize people just because
they have sought medical treatment for this condition?
How frequently does transsexualism
occur?
'Prevalence' is the number of cases present in a given population
at a given time. If there are 100 cases of some condition in
a city of 100,000, then the prevalence there at that time is
1 in 1000 (1:1000). Fortunately, we can make good estimates of
the prevalence of transsexualism without being a research scientist.
Any good journalist could easily triangulate on good ball-park
estimates.
Medical authority figures often quote a prevalence of 1 in
30,000 for MtF transsexualism and 1 in 100,000 for FtM transsexualism.
You'll see these numbers over and over again, as in recent news
stories in the Washington
Post and the New
York Times. But don't these figures seem odd to you? They
portray transsexualism as being incredibly rare. However, many
people nowadays know a transsexual person or know
of one in their school,
company or small community. Where do these "extreme rarity"
figures keep coming from?
These figures are from the American Psychiatric Association's
Diagnostic and Statistical Manual of Mental Disorders (DSM-IV).
The numbers are often sent to the media by the two "elite
psychiatric centers" that have long promulgated and dominated
thinking regarding "psychiatric theories of transsexualism",
namely the Clarke Institute in Toronto, Canada and the Johns
Hopkins School of Medicine in Baltimore, MD.
However, the figures are from decades-old data when modern
sex reassignment surgery (SRS) first became available, and only
include the numbers who bravely stepped forward and asked for
SRS at a time when discrimination was incredibly intense. Common
sense says there were many more who suffered in silence than
came forward openly. But how many?
Let's do some "numerical detective work". We can
triangulate the prevalence of MtF transsexualism in the U.S.
by estimating how many transsexuals here have already had SRS.
We can then divide that number by the population of adult males
in the U.S. (up to about age 60, since those older had little
access to the surgery in the past).
Before 1960, only a tiny handful of SRS operations were done
on U. S. citizens. Georges Burou,
M. D. of Casablanca, Morocco, then began doing a large series
of operations in the 1960's using a vastly improved new "penile-inversion"
technique. Harry Benjamin, M.D., a U.S. physician who had done
pioneering research and clinical treatments of transsexualism,
began referring many U.S. transsexuals to Dr. Burou and to several
other surgeons who used Burou's new technique. (Lynn later learned
from Dr. Benjamin that in 1968 she had been among the first 600
to 700 transsexual women from the U.S. to have had SRS).
Harry Benjamin, M.D.
The great medical pioneer and compassionate
physician
[photo taken by Lynn Conway in
1973]
The U. S. numbers grew in the 1970's as gender-identity programs
at Johns Hopkins and Stanford University triggered an easing
of restrictions on SRS in U.S. hospitals, and several U.S. surgeons
began performing SRS. In 1973 Lynn learned from Dr. Benjamin
that 2500 SRS operations had been done on U. S. transsexual women
by that date.
Beginning with that data, the table
below shows Lynn Conway's estimate of SRS operations done
by major SRS surgeons both here and abroad on U. S. citizens
in recent decades, extrapolated to include those done by many
secondary surgeons (each performing smaller numbers per year).
A range of values is given, from conservative to most likely
numbers.
At present about 800-1000 MtF SRS operations are now performed
in the U. S. each year, and that many or more are performed on
U.S. citizens abroad (for example in countries like Thailand,
where the quality of SRS is excellent and the cost is much lower).
The top three U. S. surgeons (Eugene Schrang, Toby Meltzer and
Stanley Biber) together now perform a total of 400 to 500 SRS
operations each year. Stanley Biber alone has done over 4,500
SRS operations since he began doing the surgeries in 1969; for
many years Dr. Biber did two SRS's per day, three days per week!
"Lynn Conway's
Numbers": Estimates of MtF SRS operations among U. S.
residents:
1960's
1970's
1980's
1990 - 2002
1,000
6000-7000
9,000-12,000
14,000-20,000
Adding up these numbers we find that there are at least 30,000
to 40,000 post-op transsexual women in the U. S. Of course some
surgeries done by U.S. surgeons are on foreigners (perhaps 15%?),
and some who've undergone SRS have passed away. However, the
majority of post-op transsexuals had SRS within the past 15 years,
and a high percentage of them are still living. TS's in the smaller
group who underwent SRS in the 60's to mid-80's were mostly young
- in their twenties and early thirties, and thus most of those
women are still alive too. Even accounting for mortalities, Lynn
estimates that the number of post-ops in the US is greater than
32,000.
To determine the prevalence of MtF SRS, we simply divide
32,000 by 80,000,000, which is the number of U. S. males between
18 - 60 (the age range from which most current post-ops originated):
32,000/80,000,000 = 1/2500.
We discover to our amazement that at least one out of every
2500 persons born male in the U. S. has ALREADY undergone SRS
to become female! This 1:2,500 estimate is vastly higher than
the 1:30,000 estimate so oft-quoted by the medical community.
The DSM-IV number is clearly way off, and by at least a factor
of 12! However, on closer examination we will find the error
is far worse than even that!
But remember: The DSM-IV "estimate" is for the
prevalenceof transsexualism, not the prevalence
of SRS. Recent newspapers articles always make that interpretation,
and refer to the 1:30,000 figure as a "the number of transsexuals".
Lynn estimates at least 3 to 5 times as many people suffer
intense MtF transsexualism as those who have already undergone
SRS. The reasons are obvious: Many transsexual people are unaware
of the options and treatments for resolving the condition, and
suffer in silence thinking there is no hope. Many are terrified
to "come out" and seek help for fear of social stigmatization.
Many more are incapable of paying the high medical costs for
transition. Thus there must be on the order of 100,000 to 200,000
UNTREATED cases of intense transsexualism in the U.S.
Thus the number of treated and untreated cases must be ~
130,000 to 240,000. If the number were 160,000, which is nearer
the lower end of this range, then the prevalence of intense transsexualism
is ~ 160,000/80,000,000 = 1:500. This value is only a rough LOWER
BOUND on the prevalence, and the intrinsic value could easily
be much higher.
These studies begin to triangulate on a likely prevalence
of intense MtF transsexualism in the range of 1:500 to 1:250.
This is roughly 100 times the number (1:30,000) published by
the APA in the DSM-IV-TR! Therefore, the DSM-IV prevalence numbers
are wrong by more than two orders of magnitude*.
By comparison, consider the prevalence of other conditions
having profound impacts on people's lives: The approximate prevalence
of muscular dystrophy is 1:5000, multiple sclerosis (MS) is 1:1000,
cleft lip/palate is 1:1000, cerebral palsy is 1:500, blindness
is 1:350, deafness is 1:250, self-reported epilepsy is 1:200,
schizophrenia is about 1:100, and rheumatoid arthritis is about
1:100. All of these conditions are high on our society's radar
screen and there is massive public empathy for those who suffer
from them. There are large research funds available for studying
and treating these conditions, and patients have welcome access
to any existing medical treatments that might relieve such conditions.
Contrast that to intense transsexualism, which has an equally
profound impact upon a person's life. This socially unpopular
condition is totally off our society's radar screen and access
to effective treatment is out of reach for the vast majority
of sufferers. Meanwhile, the medical establishment is totally
unaware of the prevalence and tragic impact of the condition.
For further discussion of the prevalence of
transsexualism, and a discussion of how and why the psychiatric
community estimates are so erroneous, see Lynn's page on
With 1500-2000 people in the U.S. now undergoing MtF SRS
each year (and at least half that many undergoing FtM surgeries),
transsexualism is common enough that large schools and companies
encounter a transitioning case from time to time. Everyone knows
this. The media is full of stories of transition. Universities
in particular have seen many recent transitions among faculty
members who have tenure and who can "get away with"
open transition without losing their jobs. The numbers are now
large enough to warrant formal rethinking of school and company
policies so that such transitions can proceed smoothly and successfully.
As awareness spreads that TG and TS conditions are not all
that rare and that many young people have successfully transitioned,
it is becoming more likely that TG and TS kids will self-identify,
come out to themselves, and on average seek help much earlier
in life than in the past. It is also more likely that they'll
find help, because more psychologists and family counselors are
now adding gender counseling to their professional services,
and because so much information is now available via the web.
However, the old myth of the "extreme rarity of transsexualism"
has led to some severe social consequences, including the conflation
of TG/TS conditions with "being gay" and the long-standing
invisibility of the many "street trannies" who
don't register on society's
radar screen, as discussed in Part I. Only as society realizes
that TG/TS conditions are not all that rare will these conditions
be taken more seriously.
Numbers count! They really do matter! Well-triangulated ballpark
numbers provide far better social measuring sticks than reliance
on the uninformed, non-common-sense, self-serving propaganda
of a biased professional group (the psychiatrists) that a has
a vested interest in "low numbers" and "non-permissiveness"
towards transsexualism. Physicists, engineers, epidemiologists
and politicians know that getting "good numbers" really
matters, and can affect major scientific, engineering, social
and political decisions in the real world. It's about time that
psychiatrists were confronted with the reality of the widespread
nature of TG and TS conditions.
How is MtF transsexualism medically
treated?
Whether it is hard-wiring in the brain, or structures deeper
in the CNS or some other mechanism that causes innate gender
identity, one thing is for sure: Gender identity cannot be altered
by psychological or psychiatric treatments under the old "mental
illness" model. Countless TG and TS people have been subjected
over the decades to psychiatric "treatments", including
shock therapy and institutionalization, and there are no confirmed
cases of any "cures" that way.
However, dramatic modern medical and surgical advances have
made it possible for the gender-identity conflicts of intense
transsexuals to be fully corrected. By undertaking female hormone
therapy and undergoing sex reassignment surgery (SRS) to change
the genital sex, the body-sex can be altered to match the neurological
sex, thus solving the MtF transsexual's gender incongruity. These
treatments are usually conducted under the guidelines defined
in the "HBIGDA
Standards of Care, Version Six" of the Harry Benjamin
International Gender Dysphoria Association.
In the past, many trans women
were forced to see psychiatrists, who served as strict "gatekeepers" to all
aspects of transition. They claimed that their permission was required for
hormones, for social transition and for SRS, and it often was granted only
after years of "therapy". Unfortunately, by thinking of transsexualism as a
mental illness, and having little knowledge of the many practical aspects of
transition, such psychiatrists proved to be very poor gender counselors.
Today it is much more common for transitioners to obtain help and advice
from well-informed, specialized gender counselors who can actually help them
succeed in transition.
Prior to SRS, the transitioner completes a period of hormonal feminization
and social transition to living full-time as a woman. After some
time has passed (usually a year or so) and the person is
still sure of their feelings about
complete transition, they then undergo SRS. In this surgery the
external male genitalia are removed and portions of those genital
tissues are used in the construction of female genitalia, including
a sexually functional vagina and a sensate clitoris. The basic
SRS operation is often followed by later "labiaplasty"
surgery to refine the external appearance of the new female genitalia
by shaping normal-appearing inner and outer vulvar labia. The
appearance and function of the reconstructed genitalia are virtually
indistinguishable from those of women who were born with typical
female genitalia. A thorough discussion of the historical development
and surgical details of MtF SRS is contained in Lynn's
SRS webpage. Many post-operative MtF transsexual women continue
to enjoy strong genital arousals and can enjoy vaginal sexual
intercourse just as any women does. Many post-op TS women are
orgasmic; some are highly so (see discussion of arousal and orgasm
in post-op women in Lynn's SRS webpage).
Unfortunately, most people are unaware of the nature of sex
reassignment surgery, and mistakenly believe that it involves
only the removal of the male genitalia, as in the cases of the
Hijra of India. Such ignorance fosters
many superstitions and prejudices about post-op MtF transsexuals,
especially concerning their sexuality and sexual behaviors (many
ignorant people assume that post-op women are limited to anal intercourse, not
understanding that these women really do have a vagina). However, there are
now many web resources covering all aspects of SRS, and such ignorance is
becoming less common in the general population.
Ongoing treatment with female sex hormones (especially after
SRS) greatly alters body sensations, emotional feelings and secondary
sex characteristics, including stimulating growth of breasts,
softening of the skin, redistribution of fatty tissues, and so
forth. Over time the effect can be a startling and rather complete
physical transformation from being a boy into being a woman.
Released from the misgendering trap, the new woman can find emotional
healing and self-acceptance, and can go on to live a real and
joyful life.
For more detailed information about these physical
gender transformations, including diagrams and photographs, see
Lynn's webpage on
TS transition is a term used by transsexual people for the
period of time when one is undergoing a "change of social
and physical gender". For the young street tranny, transition
usually means TG transition, i.e., the taking of female hormones
to feminize her body and then beginning to live openly as a girl. Sadly, because of employment difficulties,
in many cases such girls may be able to only aspire to living
life as a transgender woman, without SRS. For other TS transitioners
who have better financial opportunities, such as middle-class college students and well-employed adults, transition means the same
thing - but with the added goal of achieving a full change of
physical gender through sex reassignment surgery (SRS) and then
going on to a full social assimilation as a woman.
In an era when transsexual women are still highly stigmatized
in many communities, the infrastructure that supports TS transitions
is very analogous to the "Underground Railroad" in
the U.S. which helped African-American slaves escape from the
South. As discussed in the NPS
website and National
Geographic website, "the Underground Railroad was neither
'underground' nor a 'railroad,' but was a loose network of aid
and assistance to fugitives from bondage. Perhaps as many as
one hundred thousand enslaved persons may have escaped in the
years between the American Revolution and the Civil War."
In much the same way, a modern network of care providers including
specialized gender counselors, electrologists, endocrinologists, surgeons, attorneys
and many others, quietly and rather secretly provide aid and
assistance to those seeking escape from the bondage of their
birth-sex. In this case, most escapees hope to assimilate
after their escape from bondage, so that their origins are concealed
and they can be "fully free". This degree of escape
is very analogous to that of an escaped slave from the South
before the Civil War who was lucky enough to "pass for white"
in the North and then be fully welcomed into the majority white
society.
Sadly, there is a psychic price to pay for "passing
in stealth" for the TS woman - as there was for the escaped
slave who passed for white - namely the loss of contact with
past friends and family, and the constant fear of being outed
and losing everything in one's new life. However, for
some this may be a very
small price to pay for freedom from bondage and the opportunity
for a full human life.
A complete transsexual transition from male to female (including
SRS) usually takes at least two or three years, and often longer.
The process begins with guidance and counseling, peer support,
and then the initiation of hormonal feminization. The effects
of estrogen, taken in large pre-operative doses, are subtle but
quite profound as the skin softens, breast begin to develop,
and fatty tissues gradually redistribute into a more female pattern.
Electrolysis is also begun to remove facial hair and conspicuous
body hair. Electrolysis is a very painful, expensive, time-consuming
process in which little needles are inserted into the hair follicles
and then heated to kill them. It often takes 100 to 200 hours
of electrolysis to remove just the male facial hair. The
process causes many logistical and time-management problems for transitioners, because the facial hair must be allowed to grow
out for a day in order to treat it - and the treated areas are
often red and irritated for a day or two afterwards. However,
unless all dark facial hair is removed, the new woman has no
chance of "passing", because those hairs show beneath
the skin even when fully shaved and covered with foundation.
Until facial electrolysis is completed, transitioners usually
resort to using special concealment makeup such as Covermark
or Dermablend. These
makeup systems are designed for people who have serious skin
discolorations such as birthmarks. They will temporarily conceal
well-shaved dark hairs without looking "too thick",
and have long been used by gay drag performers and other "female
impersonators" to feminize their facial appearances. However,
most transitioners try to get far into their facial electrolysis
before attempting their social transition into RLE, in order
to minimize the impact of electrolysis on their work schedules,
minimize their dependence on cosmetic concealment, and improve
their chances at passing well.
Before and during RLE, many transitioners also undergo surgeries
that further feminize their facial and body appearance, especially
by reducing masculinized facial bony structures (protruding brow-bulges,
jaw bones and chins). Some of these medical procedures, such
as facial feminization surgery, are often extremely painful,
and the TS girls must steel themselves to this very traumatic
aspect of gender transition.
However, there is far more involved than just these medical
and surgical treatments. The MtF transitioner must completely
and permanently change their social gender. In addition to learning
how to dress and make up and be pretty as a woman, she must also
readjust a phenomenal range of mannerisms and gestures, and learn
a whole new set of social protocols. Once she starts this journey
and her appearance begins to change in noticeable ways, many
people will be afraid to associate with her, or even be seen
with her, until she gets far enough along to "pass".
In most cases, she must finally leave her past life behind
- often breaking all ties with friends and family as she moves
on into her new life - much as did early immigrants from foreign
lands, and indeed much as did escapees from the bondage of slavery
in the South in the 1800's.
Only just so much assistance can be gained from gender counselors,
medical service providers and peer support groups. Thus most
of the responsibility for planning and implementing this complex
journey rests with the transsexual woman herself.
Therefore, a transsexual gender transition is a very major,
socially disrupting, emotionally traumatic undertaking, and is
indeed one of the most difficult things someone can do. Traveling
this path can be a very lonely journey, because all the physical,
emotional and social challenges along the way must usually be
faced alone, without much help from family and friends. However,
escape from a body and the daily entrapment of a gender role
that feels totally alien to you is very much like escape from
bondage. Any TS girl who can see a path to full gender transition,
no matter how painful or difficult that path is, will usually
make her run for freedom.
Fortunately, there are now many websites containing valuable
information about these many dimensions of TS gender transition.
These excellent guides reveal the underground railroad of services
and care-providers who can help the transitioner at various stages
of her journey. The very best of these websites is Andrea James'
"TS Roadmap".
Andrea is a beautiful, successful post-op woman. Her site contains
a wealth of knowledge, and is now the "Bible" of male-to-female
transition.
The most complete guide to MtF TS transition on the
web is Andrea James' "TS Roadmap". Anyone contemplating
transition should carefully study Andrea's site, and use it as
the basis for their transition plan
As transition proceeds, hormonal feminization causes
not only visible physical changes, but also enhances subtle yet profound
psychic changes. Under the influence of estrogen (especially after SRS), it
becomes easier to shift one’s basic "inner vibes" from any vestiges of
“vigilant masculinity" (especially a non-smiling "tight" face and avoidance
of eye contact) to that of "warm femaleness" (with its projection of
non-threatening vulnerability, especially via a warm, open-eyed smile). Here
are some tips from Lynn about this important "inner psychic transition":
"While in the male role, social pressures reinforce a
tendency to always "keep an eye out" and "keep some distance" between
yourself and others. To guys it sometimes seems as if a "fight could break
out at any moment" and they must always be on guard. It is very important
during gender transition to phase out any remnants of such feelings.
Relaxing and letting oneself feel vulnerable and open, and then smiling
warmly, will help this inner transformation proceed.
Perhaps for the first time you’ll fully open up to
your inner female feelings, now enhanced by estrogen. You’ll begin to
experience a profound shift in inner emotional setting towards wonderfully
soft warmth and vulnerability, and openness towards warm emotional contact
with others. As this happens, you will “vibe” differently not only inside
yourself but to others too. The warm social feedback you then receive as a
woman will then reinforce your new internal feelings.”
Other people unconsciously read gender "vibes" just as
they unconsciously read masculine facial features, and even very pretty
transitioners may not seem female if they still "vibe" as males. Thus it's
important to project one’s inner feelings as early as possible during
transition. Otherwise, negative social feedback from others can stall
progress towards self-acceptance and self-realization - enclosing the
transitioner in a vicious circle of resentment and rejection.
Fortunately, the hormonal changes during transition
tend to reinforce these inner emotional changes. But this can be scary too.
At the beginning of transition, persons are often quite fragile. Many become
much more emotional than before, with emotions and tears coming much more
easily, and they need to be reassured that this is a normal response.
Often they are a lot more open, talkative and interactive too. Sometimes
for the first time in their lives transitioners are accepting and asserting
themselves, and not hiding their true self or their pain at having to play a
false role in the past. This is a profound experience for the transitioner.
These changes can be so pronounced that friends, family and loved ones may
become “lost” (confused by it) for a while.
It can take time for a transitioner to completely get
rid of the mask she had to wear and the pressures she suffered under,
sometimes for decades. Even though most transsexual women never really
corresponded to the stereotypes of masculine behavior society tried to
impose on them, most were subjected to extreme pressure to conform to those
stereotypes. Their
burden was often most painful during childhood, when they were less able to
resist pressure, and when they felt totally alone and betrayed and tormented
by those whose duty it was to protect them. Such
experiences can have devastating consequences and cause lingering sadness in
some cases. However, a carefully chosen, really helping, respectful,
welcoming and loving therapist, one who places him/herself as a guide and as
an ally (instead of a gatekeeper) can help a lot with issues like this, as
with many other aspects of the transitioner’s journey.
In the end, it is by discovering and fully manifesting
their true inner selves, and leaving behind unwanted vestiges of their
pasts, that most MtF transitioners' identities as women become obvious to
everyone.
Voice training:
Another very difficult step for many TS transitioners is
adjustment of a deep masculine voice to that of a female. Here
are some tips from Lynn:
"I gradually raised my voice while I transitioned until
the fundamental tone was up to around 180 Hz. Then I worked on
making it "breathy" or "smoky" and kind-of-sexy
in sound, patterning somewhat on the voices of old-time actresses
June Allison and Lauren Bacall. I got in the habit of occasionally
checking my fundamental frequency by hitting the piano keys F
(175 Hz) and G (192 Hz) below middle-C to make sure I stayed
above 180 Hz. I recommend that you do this too once your voice
is raised.
In this range of frequencies the voice can pass as
either male or female depending upon whether it is soft and breathy
and uses female intonations, or hard and monotone (male). Thus
you can work on getting your frequency up into this range and
keeping it there, even when still presenting as male. The adjustment
to female is then made by using intonation and a "breathy"
form of voice.
Once you've permanently transitioned, try to raise your fundamental
frequency further towards middle-C (262 Hz). If you can raise
your voice closer to middle-C, it will be within a female-only
range and will be a great asset to you.
Whatever you do with
your voice, the key test of success is whether you can always
pass as female with strangers on the telephone (i.e, whether
you are always called "ma'am" by those who can't see
you and only hear your voice). If that always happens, then your
voice is OK. If not, then you MUST keep working on it!"
When Lynn transitioned decades ago, we TS women had to struggle
on our own to develop our voices by trial and error, judging
from sometimes harsh feedback from strangers whether we were
doing OK or not. Nowadays there are excellent instructional materials
available to help you develop your new voice. Transitioners can
now benefit greatly by studying and participating in the exercises
at the TS Voice website.
I also strongly recommend that transitioners purchase and carefully
study Andrea James' and Calpernia Addams excellent new video
training course entitled "Finding
Your Female Voice" (available in VHS and DVD).
Following the success of that video training course, Andrea
and Calpernia have gone on to produce a two-DVD training course
(also available on VHS) entitled
Becoming
You: The Fast Track To Your Female Face.
This new course for TS women covers make-up and presentation,
including sections dealing with scalp hair loss and hairline
issues, managing hair removal, sections on clothing, shoes, jewelry
and accessories and on dealing with the emotions and social situations
surrounding the process of transitioning. Here are some quotes
from Andreas and Calpernia about their new course:
"Most makeup instruction available in the TG community
is designed for the women who "dress up" for kicks.
That's cool, but we are focusing on being accepted as female
in day-to-day life. This is designed for women like you, who
wish to have a smooth transition into living full-time in mainstream
society. - - - While the tone of this video is upbeat and fun,
I know this isn't just fun and games for you. You're making a
serious commitment to transition. You want to be accepted as
female in work and social settings, not just at home in front
of a mirror or in a dark bar on weekends."
This is a truly outstanding new training course. It covers
many essential skills that are very difficult to efficiently
and thoroughly learn by any other means, and it also contains
lots of positive thoughts and encouragement along the way. I
highly recommend that all transitioners purchase and carefully
study this wonderful course:
As a key step in the formal treatment protocol, the transsexual
woman enters what is often called a "Real Life Experience" (RLE). The
woman usually enters RLE only after having worked very hard during
her pre-transitional period to learn how to feminize her voice,
facial appearance and presentation, and after being on hormones
and electrolysis long enough to feminize her features.
RLE is a time when, under the guidance of her gender counselor,
she "socially transitions" into living and working
full-time in her new gender role for at least one year. RLE is a time when all her social skills, grooming, dressing
and personality presentation are enhanced and refined, and confidence
and self-esteem are developed in her new social role. It is also
a time for handling many of the difficult family, relationship,
employment, bureaucratic and legal aspects of the gender change.
Finally, it is a time for deep introspection, during which
she must make the ultimate decision of whether or not to undergo
SRS (be sure to
read the WARNING section
below!).
Illustration from cover of
Supplement 154 of the 1993 Scandinavian
Journal of Urology and Nephrology.
[Note the old-fashioned notions of requiring "psychiatry" and "permission"
before going on hormones or transitioning (changing identity).
Unfortunately this is still the case in some countries.]
If the woman wants to go forward to SRS
after successful completion of at least one year of RLE, and if she is
otherwise in good health and good spirits, her gender counselor
will provide her with the needed documents so that she can go on for the surgery.
However, even after her sex reassignment surgery there are still
many, many things she must do to complete a full transition,
and settle fully into the new gender role.
Although
the procedures and trans-community customs for the social changes,
real life experience (RLE) and medical
treatments are well established, transition is often an awkward and
frightening time for the emerging woman. She must face many challenges in
relating to others, maintaining employment, and maintaining self-esteem
and confidence in the face of public ridicule, family rejection
and social stigmatization. There is always the risk of "transition
failure", where someone loses their employment, is unable
to make steady progress through all the complex medical and social
procedures, and eventually becomes socially marginalized back
into the world of the inner-city streets (see, for example, A Tragedy's Tragic End). Transition
failures often have terrible consequences, and the TS transitioner
needs to plan and work carefully to avoid such a failure.
On the other hand, tens of thousands of transsexual women
have completed successful transitions and are living full lives
as women now. Many of these women have gone on to have wonderful
love-lives and romances after their transitions. Many have found
life-long partners and many have successfully married (as in
many stories in the
"TS
Women's Successes" page). In the end, being able to
find a life-partner (whether male or female), and enter into
a loving, sensual, fulfilling relationship while at the same
time feeling fully gender-congruent in one's own body - that
is the ultimate reward for all the pain, cost and sacrifices
of TS transition.
Transitioning "On the Job"; How FFS can insure employment continuity:
Fortunately, with increasing awareness and acceptance of
transsexual transitions a number of leading companies have established
policies and guidelines that protect and support "on-the-job"
(OTJ) or transitions. Many corporations
now have (in addition to sex and sexual orientation) some form
of gender protection as part of their EEO policies,
including American
Airlines, Apple, Avaya, Eastman Kodak, Lucent, Verizon, and Xerox.
Notable
among these companies is Lucent, which has very well-defined
guidelines for such transitions. In these and many other
companies the TS woman does not have to lose her job or transfer
in stealth - she can transition while maintaining her present
position. See also the Washington Post article
"More
Transsexuals Start New Life, Keep Old Job".
In an important recent trend, many TS women schedule
facial
feminization surgery (FFS) just BEFORE their social transition
at work, in order to remove vestiges of facial-bone masculinization
caused by testosterone. This is an excellent way to insure a
really smooth OTJ transition, because it makes it ever so much
easier for co-workers to actually "see them as females".
Continuity of employment and for continuing a good career often
more than compensate for the cost of this surgery. Sally is a
good example of this approach: She transitioned OTJ just after
her FFS, and has advanced really well in her company since then.
For example, consider the case of Sally,
as seen in the following three photos. The first photo (on the
left) shows her when she was still a boy, and a very handsome
boy at that. The second photo shows her after two years of hormones
and electrolysis. Many transsexual women would feel very wonderful
having made a transition from the first to the second photo,
and by contrast many might think they "look really good
now".
However, although her facial features are softened and somewhat
feminine in the second photo, you'll notice that she still has
a "tranny appearance". The protruding brow ridge, the tall chin
and the widely flared jawbone that made her handsome as a boy
now spoil her looks as a woman. The third photo shows her after
having FFS performed by Doug Ousterhout, M.D. We now sense the
problems in the second photo and why she "wasn't pretty"
there. The FFS transformation, while subtle, is really profound.
She is now a strikingly beautiful woman, even without any makeup
on. This is an excellent outcome. Now not all results will be
this striking. However, the results are very often life-changing
in their impact on passability and self-esteem.
Pretransition; after two years
on hormones and electrolysis; after FFS with Dr. Ousterhout
Well, what on earth is going on here? What made Sally's appearance
change so much? The answer is seen in PROFILE views. Although
we almost never look at ourselves in profile, that's the direction
other people often see us from. And it is our facial profile
that most determines facial beauty and gendering at intermediate
angles towards face-on. Thus it is a male-type profile that most
frequently gives away "tranny features" and keeps a
TS woman from looking pretty.
The following profile photos of Sally show the truly astounding
changes made by FFS. Her appearance in profile before FFS was
very unflattering for a woman, even though she looked "OK"
face on. After FFS her protruding brow ridge is gone, and is replaced
with a rounded female contour. Her nose has been reshaped and
contoured into her reshaped forehead. Her chin height and chin
angle have been radically modified. The width and flare of her
jawbone have been greatly reduced. And her hairline has been
brought forward significantly:
Profile views of Sally before
and after FFS:
Sally finally has facial features similar to those she might
have had if she'd gone through her initial puberty as a girl:
on estrogen and without testosterone. The final results are wonderful
and are truly life-changing, as seen in the following photo.
These results also indicate how important it is for our society
to help transsexual girls earlier in life - so they could avoid
developing heavily masculinized facial features which require such costly and
painful surgery to correct.
Sally - now a beautiful woman
It is no wonder that
Sally
had a smooth OTJ transition after her FFS. As you can imagine,
success in maintaining a good job and in continuing to advance
in a good career can have a huge impact in a transitioner's life,
and thus careful planning on how to do this can be critical for
overall success in transition. Warm acceptance at work can then
be followed by an ever-increasing spiraling outward into new
social relationships, and out into a fuller life in one's new
identity.
Join transition authority
Andrea James and famed Facial Feminization
Surgery pioneer
Dr. Douglas Ousterhout for an illustrated
conversation about his procedures at the California Pacific Medical
Center. It's just like being there!
If you're considering Facial Feminization Surgery, shopping for
surgeons or just informing yourself on the procedures, this seminar
is for you.
Characteristics that no current
surgery or treatment can transform:
The above cases
and photos illustrate how spectacular and life-changing facial feminization
surgery can be. However, there are some things that cannot currently be
corrected. For example, no medical procedure can transform a very tall and broad-shouldered person into a petite and slender one.
Trans women who are
taller and have broader shoulders than the majority of women need to find ways
of accommodating to and even exploiting their physicality in various ways.
Becoming at ease with our bodies is very important, not only for a successful
transition, but also for happiness in life beyond transition.
If tall trans
women look around them, they will discover many other tall women who can serve
as very positive role models. They prove that a woman can have a fulfilling and
happy life independent of her height. Finding these role models will reveal that being tall and
perhaps a bit athletic can be very positive
and attractive features for a woman, especially if she keeps herself quite trim
and in good shape.
There is also
an extensive infrastructure of websites and retail outlets that cater to tall
women, and that can help a tall woman look her best.
Tall women can thus enjoy shopping and fashion as much as any other
woman, and have the opportunity to find superb clothes that are high quality and
are as business-like, or as elegant, or as "practical" and sporting, or as full of fantasy
and as feminine as they want.
Furthermore,
there are many tall men's and women's clubs and singles groups, where tall girls
will feel short by comparison to the men! There are also many
potential partners who enjoy being with a tall, self-reliant woman who, for
example, enjoys the out-of-doors and is a good sport when doing active,
adventurous things. By following and exploring a variety of such pathways,
a tall girl can find many friends, companions and dating partners, and go on to
live a full and happy life.
In the end,
living life as a happy and radiant woman
has nothing to do with trying to correspond to a stereotype, but is related with
one's ability to welcome and cherish the woman within - then living
according to one's heart, while bringing kindness and warmth into one's
relationships with others.
At what age do TS women transition? And what does it
cost?
Traditionally, most TS women have transitioned on their own
as adults (after age 18), because of lack of parental and societal
support for earlier transition. The overall reassignment procedures
of counseling, hormone therapy, electrolysis to remove facial
hair, and sex reassignment surgery can be very expensive ($30K
to $40K) and are rarely covered by medical insurance. SRS alone
costs about $20K in the U.S. (including labiaplasty). Many must
spend even more than that for additional major reconstructive
surgeries, such as
FFS.
Madeleine, now a beautiful woman,
transitioned OTJ in a high-tech company just after FFS.
Therefore, most TS women must wait until they are at least
in their mid-to-late 20's or early 30's in order to can save
up enough money or build enough financial credit to complete
their transitions (including SRS). Nevertheless, the cost per
patient is low compared to the benefits, especially when amortized
over a lifetime: For an amortized cost on the order of $1000
to $3000 per year of adult life, the transsexual can leave all
the gender angst and emotional pain behind and move on to a normal
life in their correct gender.
Lynn has compiled a webpage listing photos and links to the
stories of many successful post-op women, in order to provide
clear evidence on the many successes out there. On that page
you'll find many examples of women who successfully transitioned
at a wide range of ages. By carefully studying their stories,
you'll be better able to visualize what is involved in TS transition
and how age is a factor in those transitions. Here are just a
few examples from Lynn's
"TS
Women's Successes" webpage:
Examples of successful women who transitioned
in their late 20's or early 30's:
Many women now try to complete their transitions in their
20's and 30's if they possibly can, especially those who have
very intense transsexual feelings and are totally positive that
they must transition. Some women may need to take longer or transition
later, especially if family situations or financial problems
interfere with their plans.
However, the extreme difficulties, risks, and fears of transition
often hold back many TS people for many years, even if they can
afford transition. This is especially true for those who are
highly masculinized as middle-aged adults, and who fear that
they'll never "pass" as women. Sadly, some lose hope,
and commit suicide along the way. A spiraling down into depression,
substance abuse and then suicide is a likely trajectory for many
unresolved cases of intense transsexualism, which is undoubtedly
the hidden explanation behind many otherwise baffling suicides.
As the stigma surrounding transsexualism has lessened in
recent years, more and more of the older, long-repressed transsexual
people are deciding that they must transition before it is too
late for them. Therefore, in recent years we've begun to see
the emergence of a rather visible group of "late transitioners".
Transitioning in their late 40's, 50's or even later, these women
face much greater hurdles than younger transitioners. They also have less time
to enjoy the rewards even if they are successful in transition.
Transitioning late in life can be very difficult, because
many cannot "start all over again" in stealth at an
advanced age. They may simply face too many family, financial
and career entanglements to be able to start fresh new lives
where they are only known as women. Many may also have difficulties
"passing" as women, because of the long-term effects
of male hormones on their bodies. They may remain easily identifiable
as "transsexuals" unless they undergo many painful
and expensive reconstructive surgeries and also work very hard
at undoing decades of male habits. In the end it may be difficult
for them to fully assimilate as a woman in society. Some insight
into these difficulties, as seen from a family member's point
of view, can be found in an essay by Stephen Gunther entitled
"My
transsexual father".
Many of the late transitioners emerge from long-term
marriages. Not only do they mourn their early years spent in the wrong body,
but they must also be aware that their marriage is likely to break up. If
they have children, they are likely to face struggles around custody and
visitation rights, and many are likely to lose all access to their children.
Finding a new partner, regardless of his/her sex, is
also likely to be difficult for later transitioners. They must face their
limits in passing and their lack of experience as a woman. There is some
risk that they will not find a new partner and they must be very
aware of it.
Those who are attracted to women may fear rejection
by lesbian women in their age group, many of whom have been politicized
against trans women in the past, and this may hold them back from seeking
relationships. Those who are heterosexual as women may never have
experienced the joy of young love with a young man as a young T-girl, which
can be a cause of deep regrets. Sadly, these women are often overly and
unnecessarily afraid of exploring relationships or dating men, because of
life-long fears of "homophobic" violence from men.
However, regardless of their sexual orientation,
some of these women will overcome their fears and go on to find partners,
often by seeking someone interested in a love-relationship involving deep
emotional sharing and intimacy, instead of focusing simply on sexual
relationships (as younger couples so often do). Such partners exist and
their own quest for a life-partner may be as long and as uncertain as the
one of transsexual women. However, in order to be successful in finding
love, the trans woman must have found enough peace, joy and self esteem in
herself so as to be able to fully partner in a loving relationship.
Despite facing many of these handicaps, many transsexual
people finally decide late in life that they must transition,
and some are able to do so very successfully. Several of the
women listed on
Lynn's
"TS Women's Successes" webpage transitioned during
their 50's, and have done very well afterwards, including Deirdre
McCloskey, Leandra Vicci, and Jamie Kaufman.
Examples of successful women who transitioned
during their 50's:
Although many late transitioners are much better off after
their transitions, there are many others who are not. Late transitioners
often have problems with very unrealistic expectations, difficulties
in objective self-assessment and effective self-improvement.
They may also find it very difficult to disentangle themselves
from marriages, families, careers and responsibilities. Thus
they can end up with a feeling of "losing everything"
during transition, while gaining little from their new lives
as women. Others, especially long-term crossdressers
(who often do not have the gender identities of women), may have
transitioned for the wrong reasons, which can lead to even more
serious difficulties in adjustment to life afterwards (see
WARNING).
Because circumstances force many
late transitioners to be "out", older and marginally-passable transitioners
have become a common media image of modern transsexualism. The larger
numbers of early and mid-life transitioners who have quietly and
successfully transitioned and are living in stealth, and who are well
assimilated as women, are simply "invisible" to the media, to the public and
even to other transitioners.
Quite a few transgender support groups now consist
mostly of intensive crossdressers, some of whom undertake TG transitions
late in life even though unsure about their chances of success. The dreary
images of some of these cases, who often linger in support groups long after
their transitions, can be frightening to young transitioners who may worry
whether they will "end up like that".
Such worries are usually unfounded, because by
seeking and finding help from appropriate support services at younger ages,
most young TS girls can transition and go on to live full and happy lives
and assimilate well into society.
Note that it is important for young transitioners to
find friends and support groups where their concerns are considered
important and where early transitions are the norm. After all, young
transitioners are at a time in life where their concerns are deeply
different from those of late transitioners. They are looking for their place
in life, are learning what it means to be in love with someone, and are
trying to become autonomous and more distant from their families, and so
on.
It is also essential that they find a group where,
regardless of their sexual orientation, the intensity of their desires,
sensations, and attractions as young women are not only welcomed and
respected, but fully validated. They must know that they have all the
chances to have a fulfilling emotional, sensual and romantic life, as would
any other woman. They need to be
reassured that their body feelings and longings for love and passion are
completely "natural and OK", and that after transition their lives can be
really sweet - including having boyfriends and getting married just like any
other girl, if they would like to do that.
For all these reasons and more,
it is important that young persons (and their families) become aware that
early transition can enable them to live almost their whole life in an
appropriate body and role, and that they must try very hard to not lose this
opportunity.
In the next
section, we'll go on to a discussion of options and methods for
transitioning early in life. (See also Andrea James' page
Transitioning Early in Life).






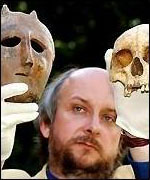
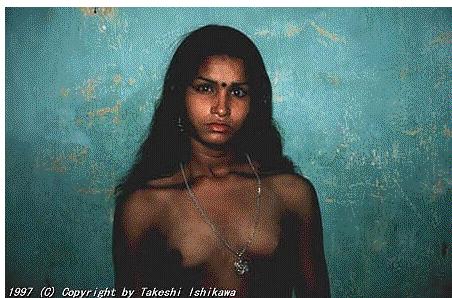
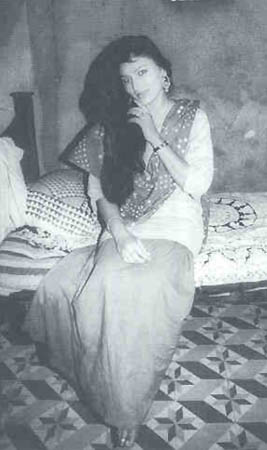
























{kind=link}