-
-
4A -WEDNESDAY MAY 24, 2000 - USA TODAY
-
Sex-Change nickname makes
Colo. town cringe: 'Nobody cares'
Transformation via surgery has
become common in community
By Pauline Arrillaga
The Associated Press
TRINIDAD, Colo. - The young waitress examined her customers
as she refilled their coffee and haltingly asked whether anyone
wanted more tea.
There was Elise, a buxom brunette in a crop top and hip-huggers.
Kate, a Harvard graduate writer in khakis, hand-knit sweater
and pearl earrings. Thea, a graphics designer sporting chic suede
boots. And Jackie, a towering figure in trousers and blazer.
In the lunchtime crowd of merchants, housewives and farmers
at the Main Street Bakery and Cafe, the four stuck out like fashion
models on a pig farm.
Retreating to the kitchen, the waitress pulled her boss aside
and stammered, "Those women I'm waiting on? They're men!"
Hardly anyone else gave the foursome a second glance. Not
in the so-called "Sex-Change Capital of the World."
Repeat that phrase to, almost any of the town's 9,500 people
and one would likely get a lecture on what the southern Colorado
hamlet should be known for - its idyllic scenery, comfortable
climate and friendly people.
Most don't mind that more sex-change operations have been
done in their town than anywhere else (about 4,500 to date);
they just hate that nickname.
"Nobody cares," says Monica Violante, owner of the
Main Street Bakery. "It's just a part of Trinidad."
Town in transition
Although no formal statistics are kept on the number of sex
reassignment surgeries, experts in the field agree that Trinidad's
Stanley Biber - because of the year he began and his age - has
performed more than anyone.
The International Foundation for Gender Education lists 14
surgeons in the USA and Canada that do the procedure, and, as
spokeswoman Sara Herwig points out, "Biber's been doing
it longer than most."
What makes Trinidad unique is not that it's the sex-change
capital of the world, but the fact that this former mining town
has come to accept its destiny, depend on it and even embrace
it.
In 1969, Trinidad was a town in transition. Coal had been
king in these parts since the turn of the century, but after
World War II, the mines began closing. By the late '60s, only
a few remained.
Families left, and Main Street, once a bustling collection
of. department stores, car dealerships and restaurants, became
a lifeless shell of shuttered storefronts.
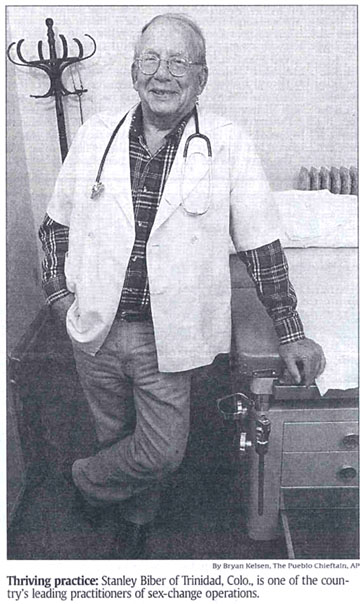
Yet Biber was thriving from his fourth-floor office inside
the First National Bank building.
As Trinidad's-s only general surgeon, Biber did it all - from
delivering babies and removing appendixes to reconstructing the
cleft palates of poor children.
Biber moved here in 1954 after serving as a MASH surgeon in
Korea and finishing a stint at Camp Carson in Colorado Springs.
In those first 15 years, Biber built a comfortable life around
a practice he loved and a town he adored. In 1969, he encountered
the patient who would forever change both.
A social Worker Biber had met asked him to perform her surgery.
"Well, of course," he told her. "What do you want
done?"
"I'm a transsexual," she replied. And Biber asked,
"What is that?"
After consulting a New York physician who had done sex reassignment
operations and obtaining hand-drawn sketches from Johnss Hopkins
University, Biber agreed to do the surgery. "She was very
happy," he recalls. "And then it started spreading
all over."
With less than a handful of doctors performing the procedure,
Trinidad became THE place to come for a sex-change operation,
and Biber was THE man to do it.
The town's sole hospital, Mt. San Rafael, was run by Catholic
nuns, and Biber hid the charts of his first transsexual patients.
But he knew he'd eventually need the approval of the hospital
board and his neighbors. Biber explained his Work to the sisters
and local ministers.
I went through the psychology of it all. They decided as long
as we were doing a service and it was a good service, that there
was no reason we couldn't continue doing them," he says.
Soon, Biber was lecturing to the hospital staff and the public.
"We figured that's his way of making a living; more power
to him," says Linda Martinez, 54, a lifelong patient of
Biber's.
Lucrative operations
Not all agree. The Rev. Verlyn Hanson, pastor of the First
Baptist Church for the past three years says the town turned
a blind eye to Biber's work because of the economic boost it
provided. "The love of money is the root of all evil, and
people will overlook a lot of evil to have a stronger economy,"
he says .
At one point, Biber's operations brought about $1 million
a year to the hospital, according to his estimates. The basic
procedure costs about $11,000, with the hospital taking in a
little more than half.
At the height of his practice, Biber performed about 150 transsexual
operations a year. His patients brought families and friends
who remained in town during their loved ones' eight-day hospital
stay.
Whether or not people liked what Biber did, they liked the
squat, balding doctor who wore jeans and flannel shirts to work
and always said hello.
At 77, Biber has scaled back his transsexual business to about
100 surgeries a year. The majority of his practice remains tending
to the ills of Trinidad's citizens. He knows retirement may not
be far off, and he's in search of a surgeon who will continue
his work. "it started here, and I want the hospital to continue
with it," he says.
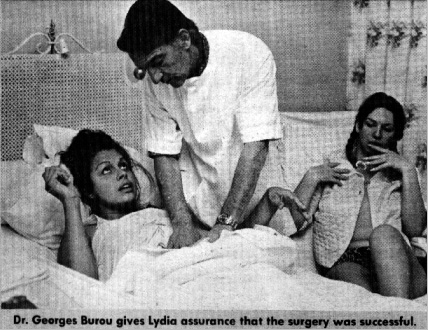
[end of AP article on Dr. Biber] |