琳À康维 著 版权@2000-2006,琳À康维。 保留所有权利。
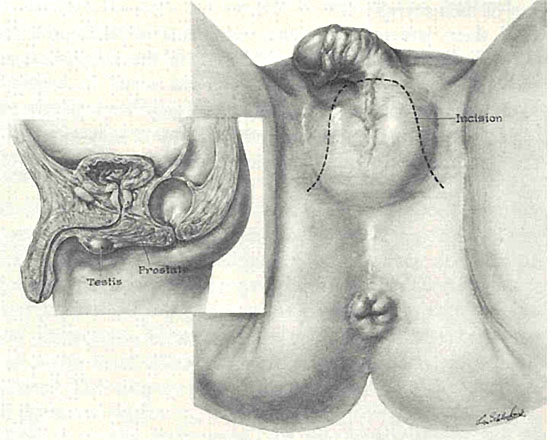
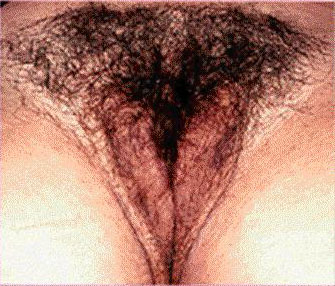
右图:一位接受了阴道成形术(SRS)和阴唇成形术的变性女人外生殖器细部(双腿由支架分开,阴唇也部分张开),主刀医生为威斯康星州尼纳市的尤金À施雷恩(Eugene Schrang)医生,医学博士。
[LC updates of 8-06-07; 7-17-09]
Deutsch, English, Espa±ol, Franþais, עברית, Nederlands, PortuguÛs, Русский,
|
 |
|
重要提示:本页面包含可能令一些读者感到震惊或极度不安的图形视觉资料以及其他医学信息。 如果你对手术神经过敏,或对自己的生殖器存在任何焦虑,请不要继续阅读。 18岁以下人士无权接触这些医学信息。进入本页,兹证明你已年满或超过18岁。 |
目 录
易性症并不是什么ô现代发现ö,相反,它是人类性别化中并不罕见和自然发生的一种变化,从古时起便被关注和记录。长久以来,包括北美土著部落在内的很多文明里,变性者可以选择穿着异性服装,以女性的方式生活,包括拥有丈夫。通过外科手术改变外生殖器以减轻强烈跨性别感觉的做法也不是ô二十世纪的发明ö。在一些文明里,甚至古文明,很多变性者自愿接受手术修正身体,以这样一种方式ô改变他们的性别ö。
阉割术的手术方法及作用在古时随处可见,它在驯养动物过程中的应用很快教会人们,在男性人类足够年幼的时候摘除睾丸也可以阻止其男性化发育。这个人将永远像个孩子ù或ô女孩子气ö。通常这种手术也会被强加到俘获的成年男性奴隶身上,以ô驯服ö他们成为ô阉人ö。对后青春期的正常男性实施这样的手术,尽管可以略微减轻其性驱动力并急剧降低发育男性肌肉的能力,却并不能改变他们的性别感受和性别认同。
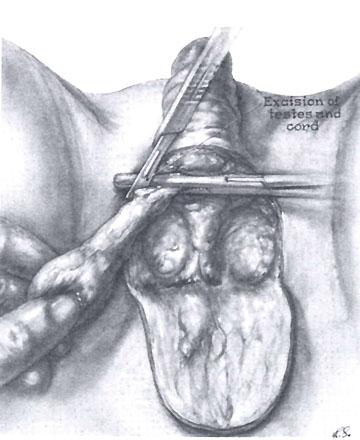
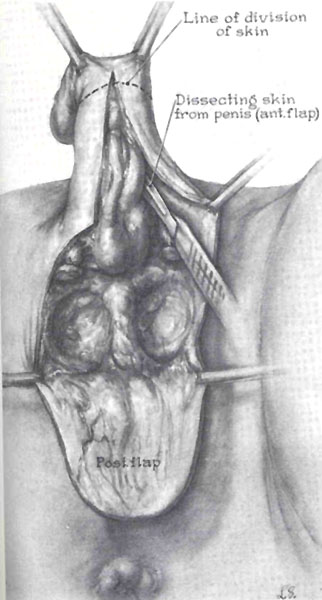
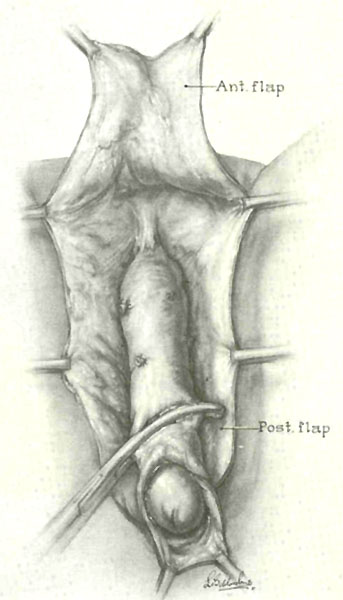
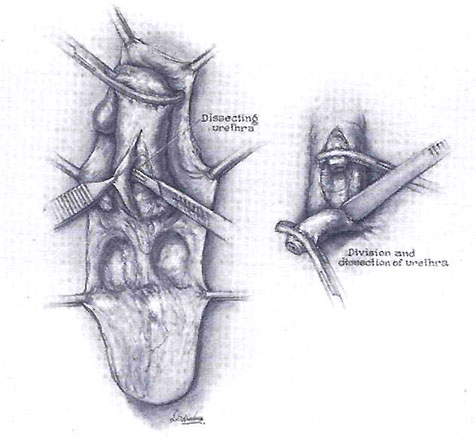
有关阉割效果的知识积累被进一步延伸,用来帮助男变女的变性者:几千年来,不计其数的变性者主动寻求和接受比纯粹的阉割术风险更大、效果也更显著的手术。在这些手术中,变性者通过睾丸、阴茎和阴囊的全部摘除而被彻底阉割。另外,阴部的外形常常被粗略地塑造成女性阴户的模样。没有人确切知道这是如何开始的,不过这种变性手术在古希腊,特别是性开放的古罗马时期就已广为人知,并常在各种ô宗教仪式ö中传统化,向经历了这种手术的ô女人ö赋予社会地位。
通过接受这些手术,由男变女的年轻变性者(如果她们幸存下来)不仅可以避免发育为男人,同时也获得了看起来与正常女性类似的外生殖器。尽管没有阴道,也缺乏女性荷尔蒙强有力的女性化效果,年轻的变性者在接受此类手术后依然能够作为女性生活得更好。
即便在今天的印度和孟加拉国,仍有众多绝望的年轻变性者离家出走,加入到ô海吉拉ö(Hijra)这个特殊的社会阶层。为了成为海吉拉,这些青少年自愿在原始条件下接受彻底的阉割手术,如同在古时一样,仅使用鸦片作为麻醉剂。多数人在10几岁青春期开始后不久便接受手术,手术效果可以从下面的照片中看到。通过及早实施阉割手术,很多人都避免了男性第二性征的发育(除变声及嗓音变低以外),而且她们的身体也能永久地保持柔软、孩童化以及女性化。
与流行的说法相反,青春期后进行彻底的外部阉割术并不一定使人ô去性化ö。青春期后完全去势的年轻海吉拉,重新获得了性唤起的感觉以及性高潮的能力。虽然这种手术心理上的冲击通常会削弱正常男性的性欲,但对年轻变性女孩的影响通常恰恰相反:手术能够使其女性知觉和性欲得到更完全的表达和释放。与现代变性女人术后的情况一样,由于体内留有残余的生殖器组织,许多海吉拉依然能够拥有强烈的性唤起感觉(即使她们没有经由现代性别重塑术而将外部神经组织保留下来,但是她们仍保留了内部的勃起组织和前列腺及其具有的间歇性高潮能力)。虽然海吉拉没有阴道,很多人仍从与男人的插入性性行为(肛交)当中(获得的高潮)享受到极大乐趣。由于经过了彻底的阉割,她们的生殖器及骨盆区看起来非常ô女性化ö,很多印度男人都很喜欢与她们做爱。相应地,海吉拉接受了她们的命运,以及有限而又实在的可能ù在其一生中作为女人找到哪怕是一点点的爱。
一位年轻的印度海吉拉,正在展示其外生殖器

塔克西À伊斯卡瓦所著
《海吉拉-印度的第三性》一书
大部分海吉拉以女性身份和其他海吉拉组成ô家族ö生活在一起,通过在婚礼和分娩的传统仪式上表演来谋生。在这个卑微而又传统的印度阶层中,很多人也从事卖淫和乞讨的行当。当今的一些海吉拉有幸获得了雌性荷尔蒙,通过促进乳房生长和女性身体曲线自然发育而使身体女性化。在青少年时期接受的阉割手术和女性荷尔蒙的共同作用下,一些当代的海吉拉变得非常美丽,不过遗憾的是,她们既没有女性性器官(阴道),也不能作为女性被社会所接受。
海吉拉的起源在印度历史中可以追溯到几百年以前,这个流传甚广的习俗,使变性者避免了青少年时期男性化发育的焦虑和命运,也为她们提供了卑微但安全的社会地位。为了ô近似地拥有女性性别ö,在充分了解自己将永别家人、余生中面对社会地位下降的情况下,这些年轻变性者在痛苦中走向极端,这反映了其内心深处性别冲突真实而又绝望的写照。
在当今的印度和孟加拉国有几百万海吉拉。欲了解更多信息,请访问金娜(海吉拉)的网站http://www.kinnar.com/和英国广播公司有关孟加拉海吉拉的报道,在塔克西À伊斯卡瓦 (Takeshi Ishikawa)所著的《海吉拉-印度的第三性》(Hijra-The Third Gender in India)一书中,可以找到很多有关海吉拉的精彩图片。一个海吉拉家族的领导者达楠 (海吉拉ô导师ö)表示,虽然被这个特殊阶层的神秘面纱遮盖了几个世纪,促使这些青少年成为海吉拉的根本原因无疑是易性症。
ô我们的性别认同危机与生俱来,它不是来自模仿或学习,而是促使我们成为女人的一种自然本能。ö-达楠
即使在当今的西方社会,极度绝望的年轻变性女孩自己ô选择成为海吉拉ö的现象也并不罕见。通过彻底地自我阉割,然后寻求医疗系统进行ô修补ö,她们因而获得了ô实施于生命早期的低成本性别重塑手术(SRS)ö。美国的很多女孩就是这么做的,之后她们服用雌激素使自己女性化,很快就变得如女孩般美丽,效果相当不错(不幸的是,阴茎和睾丸皮肤的缺失,使得以后通过性别重塑术构建阴道变得非常困难。)。在美国,更多的年轻变性女孩采取自行去势的方法来避免男性化发育,特别是在美国严格禁止医院对ô完整的男性ö实施性别重塑手术的50年代及60年代初(见下文)。
历史悠久的传统ô海吉拉式ö手术从古时一直延续至今,而且仍在印度和孟加拉等国继续使用。有关海吉拉式阉割术术后效果的详尽知识,为现代变性手术的发展提供了重要的经验背景。
[此处以后将添加:有关第一次世界大战后整形手术发展的讨论,以及1930年前后医学博士FÀ亚伯拉罕 (F. Abraham)在德国为变性女性开创性地实施阴道成形术的讨论---见:http://www.symposion.com/ijt/ijtc0302.htm#Case%201 - - -]
随着第二次世界大战后性荷尔蒙和整形手术知识的迅速发展,为易性症设计完整的医药及手术解决方案终于成为可能。在50年代,变性女性开始极大地获益于新兴的女性荷尔蒙,这些药物促进乳房发育和皮肤柔软,并随着时间的推移产生女性曲线。同样是在50年代,少数外科医生汲取了在女性两性人阴道重塑手术中的最新技术进展,开始尝试使用取自大腿或者臀部的皮片为变性女性塑造阴道。
美国人克里斯蒂À乔根森(Christine Jorgensen),是最早接受这种外科性ô性别改变ö的一小部分变性人中的一员。1952年,接受初期手术后不久她便被美国报界传媒曝光,其经历引起举国轰动。通过她的故事,很多变性人第一次了解到这种新型荷尔蒙及外科疗法的存在。然而,只有少许欧洲患者才能接受这种新型的试验性手术。
在克里斯蒂接受手术的50年代,医生们首先通过一次或多次手术摘除变性者的男性器官,随后患者需要经过一段延续期等待康复。接下来,通过近似于为两性人患者创建阴道的手术,外科医生利用取自患者大腿或臀部的皮片为其重建阴道(克里斯蒂的阴道成形术完成于1954年)。
变性先驱克里斯蒂À乔根森
早在1952-1954年间接受了变性手术

虽然患者对手术效果相当满意(特别是与她们先前的情况相比),但是这种早期的手术方法存在很大问题。移植的皮片不可靠,部分皮片有时无法ô存活ö,大块皮片的使用也令供区留下了难看的大范围疤痕。另外,大量敏感的生殖器组织在第一步手术中被永久性地切除,影响了患者性唤起的感觉和获得性高潮的能力。
从50年代末到60年代,数百名美国变性者得到了医学博士哈里À本杰明(Harry Benjamin)医生的帮助,他是一位富于同情心的内科医生和内分泌学家,在纽约市及加州旧金山市均设有办公地点。本杰明医生是第一位将跨性别认同和同性恋区分开来的医生和学者,他认为变性者实际是经受着一种原因未明的性别认知错误疾病,而不像当时的多数精神病学家那样,将变性者视为患有精神疾病的不正常人。为了减轻她们的痛苦,满足其对药物女性化治疗的强烈要求,本杰明医生开始有选择地为一些患者开具雌激素处方。同时他也对正在实施的变性手术效果保持密切关注,并开始向要求最强烈的变性患者推荐那些取得了最佳手术效果的医生。
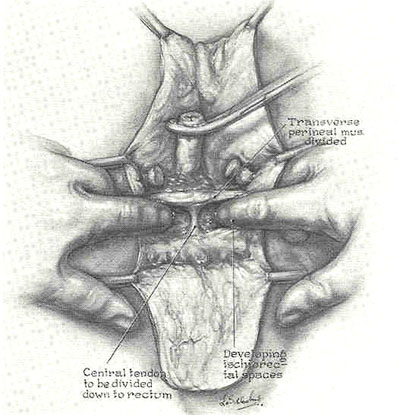
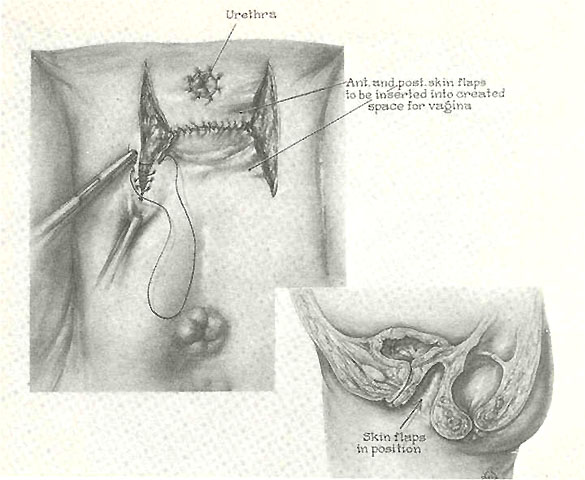
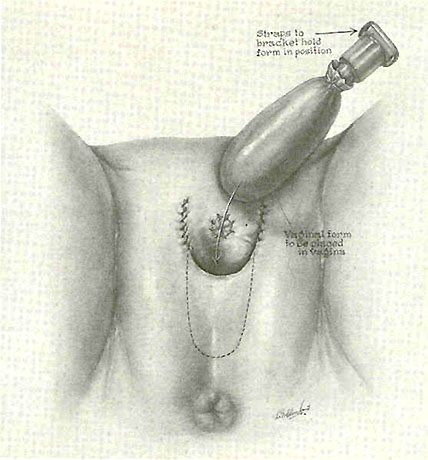
然后,在50年代末,一位名叫乔治À布罗(Georges Burou)的法国整形医生,医学博士,为男变女的变性者发明了阴茎反转男变女性别重塑手术的现代术式,布罗医生的手术方法在不断的改进中沿用至今。布罗医生的经典创新在于,利用男性性器官作为构建包括阴道在内的新女性性器官的皮肤和性敏感组织来源。
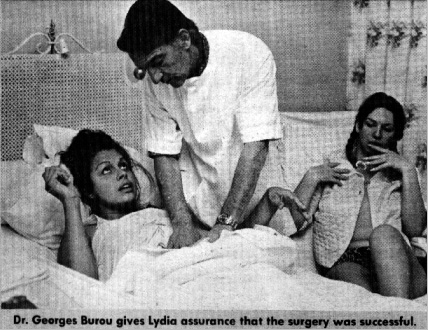
感谢法国的Pascale找到了布罗医生的这些照片
[摘自1970年7月份《国家警察公报》(一份美国男性杂志)的一篇文章]
布罗医生在其位于摩洛哥卡萨布兰卡的诊所内实施这些手术。1958-1960年间,一些来自法国巴黎拉À卡拉尔索俱乐部的出名且年轻貌美的ô反串旦角ö,包括可可西尼尔 (Coccinelle)(更多信息) ,斑比(Bambi)和艾普莉尔À阿希礼 (April Ashley),经过布罗医生的手术成功地变为女人。作为在该俱乐部工作的额外好处,许多拉À卡拉尔索女孩获得了女性荷尔蒙,她们由此变得难以置信的美丽、性感和富于女性化。有些人在性器官手术后返回俱乐部继续从事表演。她们成功的ô性别转换ö变得家喻户晓,并因此被许多显赫富有的男人作为求爱对象。一些特别富有的人(包括亚里士多德À欧纳西斯)有时会ô资助ö拉À卡拉尔索俱乐部的女孩完成变性手术,而她则会在一段时间内充当其情妇。